![]()
|
Name:____________________ Address:__________________ __________________________ __________________________ Phone:____________________
|
|
Phone Numbers Emergency:_______________ Doctor:___________________ Pharmacy:________________ Family:___________________
My Address is: ____________________________ ____________________________ ____________________________ My Phone Number is: ____________________________ |
|
Name:___________________________________________ Address:_________________________________________ _________________________________________________ Phone number:____________________________________ Age:_____________________________________________ Date of birth:______________________________________ Father's name:____________________________________ Mother's age:_____________________________________ Husband's/Wife's name:____________________________ Year you were married:_____________________________ Names of children:________________ Age:____________ ________________________________ Age:____________ ________________________________ Age:____________ ________________________________ Age:____________ Names of grandchildren: Parents _______________________ ____________ ___________ _______________________ ____________ ___________ _______________________ ____________ ___________ _______________________ ____________ ___________ _______________________ ____________ ___________ Brothers' names ________________________________ Age:____________ ________________________________ Age:____________ ________________________________ Age:____________ ________________________________ Age:____________ Sisters' names ________________________________ Age:____________ ________________________________ Age:____________ ________________________________ Age:____________ ________________________________ Age:____________ Educational Background: School Dates attended __________________________ _____________________ __________________________ _____________________ __________________________ _____________________ Work History: Place of employment Dates employed __________________________ _____________________ __________________________ _____________________ __________________________ _____________________ __________________________ _____________________ __________________________ _____________________
Hobbies: _________________________________________________ _________________________________________________ _________________________________________________ _________________________________________________
|
|
Today's Date:______________ Day of the week:______________
_________________________________ _________________________________ ____________________
_________________________________ _________________________________ ____________________
_________________________________ _________________________________ ____________________
_________________________________ _________________________________ ____________________
|
 _________________________________
_________________________________
|
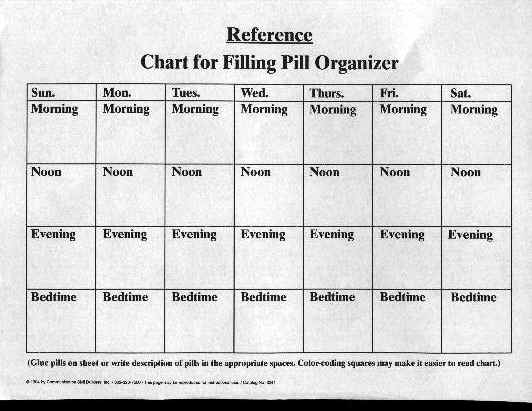
Name of Medication Reason for taking Dosage _________________ ____________________ ________ _________________ ____________________ ________ _________________ ____________________ ________ _________________ ____________________ ________ _________________ ____________________ ________ _________________ ____________________ ________ _________________ ____________________ ________ _________________ ____________________ ________ _________________ ____________________ ________ If the following symptoms occur, call the doctor: Doctor's Number:________________ ________________________________________________ ________________________________________________ ________________________________________________ |
|
Project:__________________________________ Things to purchase:_______________________ _________________________________________ _________________________________________ Things to gather:__________________________ _________________________________________ _________________________________________ Steps to complete task: 1._______________________________________ 2._______________________________________ 3._______________________________________ 4._______________________________________ 5._______________________________________ 6._______________________________________ 7._______________________________________ 8._______________________________________ |
|
Day of the week_______ Date________ Breakfast Menu Steps to complete the meal _______________ 1.______________________ _______________ 2.______________________ _______________ 3.______________________ _______________ 4.______________________ _______________ 5.______________________ _______________ 6.______________________ _______________ 7.______________________ _______________ 8.______________________
Lunch Menu Steps to complete the meal _______________ 1.______________________ _______________ 2.______________________ _______________ 3.______________________ _______________ 4.______________________ _______________ 5.______________________ _______________ 6.______________________ _______________ 7.______________________ _______________ 8.______________________
Dinner Menu Steps to complete the meal _______________ 1.______________________ _______________ 2.______________________ _______________ 3.______________________ _______________ 4.______________________ _______________ 5.______________________ _______________ 6.______________________ _______________ 7.______________________ _______________ 8.______________________
|
|
Name:__________________________________ Address:________________________________ ________________________________________ Phone Number:__________________________
Name:__________________________________ Address:________________________________ ________________________________________ Phone Number:__________________________
Name:__________________________________ Address:________________________________ ________________________________________ Phone Number:__________________________
|
|
(attach photo here...)
Name:_________________________________ Title:__________________________________ Describe the meaning of this picture:______________ _____________________________________________ _____________________________________________ _____________________________________________ _____________________________________________ _____________________________________________
|